Dr. Joel Aronowitz — Clinical Safety of Adipose Stem Cell Separation at the Point of Care

Dr. Joel A. Aronowitz , Cloe S. Hakakian BS, Ryan A. Lockhart BS
Cedars-Sinai Medical Center, University Stem Cell Center, Los Angeles CA
Abstract
Background: Pluripotential cells concentrated in perivascular areas of adipose tissue are pivotal in long term volume retention and regenerative effects of fat grafting. Unfortunately adipose stem cells are significantly depleted by all lipoaspiration techniques used to harvest fat graft[1] . Autogenous stem cells can be replenished to the fat graft in a strategy termed Cell Assisted Lipotransfer (CAL) by Yoshimura. Mounting preclinical and clinical evidence supports the rationale of CAL but routine clinical adoption of CAL in fat grafting requires a safe and predictable method of isolating adipose stem cells during the procedure in the operating room, that is, at the point of care (POC).
Mechanical, non enzymatic methods can concentrate free stem cells [2] in the stromal vascular fraction of lipoaspirate with yields in the range of a few 10,000’s cells/gram of lipoaspirate processed. Collagenase based methods however are far more efficient, consistently yielding over 250,000 viable ADSC[3] ASC cells per gram of lipoaspirate harvested. While the efficiency, cost and methodology is established, the question of clinical safety of enzymatic isolation persists.
This prospective, level 1 study reports the clinical safety of cell assisted fat grafting using a collagenase based process to liberate and concentrate autogenous stromal vascular fraction cells [4] from fresh lipoaspirate at the POC for immediate reinjection.
Methods: One hundred and sixty four subjects underwent a total of 174 stromal vascular fraction (SVF) cell enhanced autologous fat graft procedures All ADSCASC separation procedures enhanced fat graft procedures 164 subjects underwent a total of 174 ADSCASC enhanced fat grafting procedures at University Stem Cell Center between August 2009 and November 2014 for a variety of cosmetic and reconstructive indications. A standardized, non automatedmanual, collagenase based isolation process was performed at the POC in the operating room to obtain the SVF cells. The isolated SVF cells were restored tocombined with lipoaspirate fat graft immediately after isolation processing for reinjection implantation without in vitro expansion or cryopreservation storage. Detailed data concerning patient demographics, fat harvest method, separation technique, collagenase composition, process time, fat graft procedure and postoperative outcomes was collected.
Results: Cell assisted lipotransfer was performed for a variety of cosmetic and reconstructive indications. The mean time of the SVF isolation process was 91 min. Due to frequent concomitant procedures the isolation process extended the average operating room time by only 11 minutes. The mean follow-up time was 19.8 months. There were no major complications and 6 minor complications. No complications related to collagenase were observed.
Conclusions: This series of 174 CAL fat transplantation cases of CAL demonstrates that adipose stem cell isolation using a manual, collagenase based process performed at the POC does not add additional risk compared to fat grafting alone. These results provide important safety data to support expanded use of this important emerging technology in the clinical research setting.
Background:
Autologous fat grafting is an increasingly popular technique for a variety of cosmetic and reconstructive indications because it regenerates adipose tissue volume and improves radiated and damaged tissues. It is not technically challenging to perform and patients find the high safety profile, minimal level of invasiveness and donor sites appealing, but the poor predictability of volume retention still limits the full potential of fat grafting.
In 1987, the American Society of Plastic and Reconstructive Surgeons (ASPRS) issued a position paper on the use of autologous fat grafting in plastic surgery. At the time, they unanimously did not condone the use of autologous fat grafting on the grounds that “much of the injected fat will not survive, and the known physiological response to necrosis of this tissue is scarring and calcification. As a result, detection of early breast carcinoma through xenography and mammography will become difficult”1,2. Since 1987, there has been a significant body of literature that has shown that that the artifacts that resultresultant from the use of fat grafting, mainly calcifications and oil cysts, are easily differentiated from malignancy in early breast cancer screening 3–8. This has been made possible by improvements in imaging techniques as well as an expanded body of data on the subject. In 2009, the American Society of Plastic Surgeons (ASPS) published a new position paper after convening a task force to evaluate the safety and efficacy of autologous fat grafting. The task force on fat grafting determined that autologous fat grafting was a safe procedure with a relatively low rate of complications. In addition, they stated that artifacts could indeed be identified and distinguished from malignancy in early breast cancer screenings 9.
With oncological screening concerns about artifacts diminished, the remaining problem associated with autologous fat grafting is that the volume retention of transplanted tissue is variable and unpredictable. Advances in knowledge of the microenvironment of grafted tissue suggest that hypoxia is the leading cause of poor graft survivability after transplantation 10–12. It has also been noted that after harvest the lipoaspirate tends to be relatively deficient in progenitor cells compared to intact adipose tissue. This is becausehas been attributed to the fact that a large population of the stromal vascular progenitor cells tend to be located around the larger vasculature within adipose tissue, which and areas containing larger vessels tend to be avoided during all liposuction and harvest techniques 13. In addition,Additionally, part of the progenitor cell population is released into the fluid portion of the lipoaspirate, which is discarded before grafting 14. As has been demonstrated in a large body of literature, these progenitor cells,an important fraction of these progenitors termed adipose-derived stem cells (ADSCASCs), [5] have the ability to produce a variety of growth factors as well as differentiate into a variety of different cell types 15–20. The combined multipotency and growth factor secretion of ADSCASCs ASCs gives them very promising potential for use as regenerative cells, with some people even referring to them as adipose-derived regenerative cells[6] instead of stem cells.
In 2006, Yoshimura and colleagues proposed a modified fat grafting technique, called cell-assisted lipotransfer (CAL), which offers a potential solution to the issue of poor volume retention 21. The CAL technique involves supplementing the existing lipoaspirate derived fat graft with stromal vascular fraction (SVF) cells isolated from excess lipoaspirate. The stromal vascular fraction is a heterogenous mixture of cells resulting after collagenase digestion of lipoaspirate. SVF contains both white and red blood cells, as well as, vascular endothelial cells, macrophages, pericytes, and a heterogenous population of progenitor cells (ADSCASCsASCs) 22. By supplementing the fat graft with SVF cells, a progenitor rich fat graft is created which has been shown to increase the regenerative potential and volume retention in fat grafting. SVF is used in place of a pure ADSCASC population because it is more feasible for use in the clinical setting. In order to generate a more pure population of ADSCASCs from the other cells found in SVF, ex vivo culturing is required, which takes weeks, meaning the patient would require two separate procedures as opposed to only one. While studies have used an ex vivo cultured ADSCASC fraction to augment autologous fat grafting, it was not deemed to be more effective than enhancement using SVF cells 23.
The primary method used to isolate SVF cells from harvested lipoaspirate is through enzymatic digestion with collagenase. While more expensive than other techniques, collagenase has proven to be the most efficient method of isolation, yielding the highest cell counts of any reported method. Collagenase in is an enzyme which digests collagen, the primary component of the extracellular matrix which holds the adipose tissue together. Most collagenases used for clinical purposes such as tissue digestion are produced by the bacterium Clostridium histolyticum. These collagenases used for adipose tissue digestion are a mixture of two different isoforms of collagenase derived from C. histolyticum, collagenase type I and collagenase type II 24. Type I collagenase has a higher substrate affinity for the large, intact triple-helical collagen strands, while the Type II collagenase will preferentially digest the smaller collagen fragments generated by Type I collagenase 25,26. Bacterial collagenases are used instead of animal/human derived collagenases because they are cheaper to produce, but more importantly, exhibit higher substrate specificity for native collagen and collagen fragments than vertebrate collagenases 27. Safety concerns arise from the use of collagenase for ADSCSVF isolation because it is theorized that a high residual collagenase level could lead to unforeseen complications or unwanted tissue degradation in vivo after the isolated stem cellscells are recombined with the graft material and transplanted.
While there is a significant body of literature demonstrating the beneficial effects of cell-assisted lipotransfer, one of the main barriers that keeps this technique from becoming more widely used is the a lack of adequate safety data. Safety concerns of CAL arise concerning the enzymatic method used to isolate stem cells. In this study, we analyze the methods used and safety results of cell-assisted lipotransfer cases for which ADSCSVF cellss were manually isolated using collagenase at the point of care and injected immediately.
Methods:
Overview:
At a single center, 174 indications of cell-assisted lipotransfer in 164 patients between August 2009 and November 2014 were conducted under IRB approval in this prospective, level 1 study. Lipotransfer procedures were conducted for a variety of implications indications (Table #1) including breast reconstruction (Figure 1 a,b), breast augmentation (Figure 2 a,b), facial aging (Figure 3 a,b), correction of lipodystrophy and contour defects (Figure 4 a,b), chronic wound and scar treatment (Figure 5 a,b,c), and buttock augmentations. Safety and complication rates were monitored throughout. Detailed data concerning subject health, fat harvest, separation technique, process time and postoperative outcomes were collected (Table 1).
Lipoaspirate Harvest:
Adipose tissue harvest was done under general anesthesia in the operation room. Local anesthetic (lidocaine 1% with 1/100,000 epinephrine and Marcaine 0.5% with 1/200,000 epinephrine) solution was injected into the adipose tissue. Liposuction procedures were performed using standard of care techniques. With the patient under general anesthesia, adipose tissue was suctioned using a 3mm blunt cannula attached to a syringe, and an FDA approved Wells Johnson Aspirator II apparatus.
SVF isolation:
A non-automated collagenase based isolation was performed by a technician in the operating room inside of a clean biohood to avoid contamination. Lipoaspirate was first washed 3 times using a lactated ringer’s solution (130 mmol/L Na+, 109 mmol/L Cl-, 28 mmol/L lactate, 1.5 mmol/L Ca2+, 4 mmol/L K+) over a period of 10–15 minutes to remove contaminating blood cells and tissue debris. Lipoaspirate was then incubated with 35 Wünsch Units (U) of collagenase per 50 cc of washed lipoaspirate. Lipoaspirate was incubated with a mixture of clostridial collagenase type I and type II (60% type I, 40% type II) [7] resuspended in warm (37 ºC℃) lactated ringer’s solution in a temperature controlled shaker at 200 rpm for 20–30 minutes at 37 ºC℃. SVF cells were separated from the digested adipose tissue via centrifugation at 2,000 rpm for 10 min. Isolated SVF cells were then washed a minimum of 3 times using lactated ringer’s solution to adequately remove any residual traces of collagenase enzyme. The SVF cells were then brought to a final volume between 5cc and 25cc (11.8cc on average) using lactated ringer’s Ringer’s solution and returned to the surgeon for injection. A small sample of SVF cells (0.1–0.2 cc) was analyzed using a cell counting device to determine the ADSC cell yield and cell viability of the isolated fraction. (Table #1)
Graft preparation and injection:
Freshly isolated SVF cells were returned to the surgeon and recombined with graft material shortly before injection. Cells were injected into a variety of locations using a Cytori Celbrush™ injector tool with a small (?(2 mm) blunt tipped cannula using a layered technique to ensure even distribution of graft material throughout the recipient site, in a manner identical to a normal fat grafting procedures.
Results:
The average age of the subjects in our study was 52.2 years old, with an average BMI of 23.4 kg/m2. An average of 180cc of lipoaspirate was used for isolation of SVF cells. The non-automated, collagenase based isolation method took an average of 91 minutes to complete. The average graft volume was 223cc, but varied from 8cc to 500cc depending on the implication, with buttock and breast augmentations requiring larger amounts of fat, while facial procedures only required a small amount. The average follow-up time was 19.8 months.
Overall, there was a very low complication rate reported in this study (3.7%). First, there were no complications reported pertaining to the use of collagenase and no complications due to error in the operating room. In terms of the outcomes of the fat grafting, there were 0 major complications (0.0%), and only 6 minor complications (3.7%) were observed. Three oil cysts were observed (1.8%) and 3 other complications were observed that were deemed unrelated to fat grafting (1.8%) (Table 1). The complication spectrum of SVF-enhanced autologous fat grafting is the same as that associated with normal fat grafting. The occurrence rates of complications were similar, if not lower, than those associated with normal fat grafting. We have cell count data for 83 patients. The average number of cells isolated per cc of lipoaspirate was 1.99 x 105 cells/cc[8] .
Discussion:
Enzymatic v. Non-Enzymatic Isolation:
When it comes to isolation of SVF cells, enzymatic methods using collagenase have proven to be much more effective in terms of cell recovery. Collagenase is better at disruption of the extracellular matrix which holds together the adipocytes and ADSCthe surrounding stromal vascular fraction containing ASCs. By disrupting the ECM, enzymatic methods allow for a greater separation of ADSCSVF and consequentially ASCs from the adipose tissue. Various studies have published data pertaining to the cell yields achieved using collagenase digestion. In general, cell yields tend to fall within the range of 100,000 ADSCSVF cellss/cc to 500,000 ADSCSVF cellss/cc of tissue when using collagenase 13,22,28–30. From the 83 patients that we have cell count data for, we the mean number of viable cells recovered was averaged 199,000 cells/cc of lipoaspirate processed (Table 1).
In a 2014 study conducted by Markarian et al which compared various digestion processing methods for SVF isolation, both enzymatic and non-enzymatically based, use of collagenase digestion was shown to be the most effective in terms of cell recovery 29. Markarian et al. reported about 350,000 cells/cc of lipoaspirate processed when using collagenase. Another method that they examined was a non-enzymatic method which involved only centrifugation of lipoaspirate at either 800xg or 1280xg. At both speeds tested there was shown to be dramatically less cells isolated per cc of lipoaspirate, with only about 10,000 ADSCcellss being recovered per cc of lipoaspirate. Furthermore the composition of the cell populations recovered from simple centrifugation has a greater frequency of peripheral blood mononuclear cells, and therefore is not likely to be of equivalent efficacy in the enhancement of fat graft. They did report in this study that there was no significant difference in cell viability observed between the various methods.
In 2014, Raposio et al. proposed a new method for ADSCSVF isolation which does not require the use of any enzyme 31. This method involves shaking the adipose tissue in a vibrating shaker for 6 minutes at 600 vibrations per minute and then centrifuging to isolate the SVF cells. Raposio et al, reported that using this method that they were able to isolate around 6,250 cells/cc of lipoaspirate.
In 2009, Baptista et al. published data pertaining to another non-enzymatic method 32. In this method, lipoaspirate is incubated with red blood cell lysis buffer at 37 °C for 15 min and then centrifuged for 15 min. They reported an average yield of about 24,000 cells per cc of lipoaspirate processed. This was supported by Shah et al. in 2013 who reported an average of 25,000 cells per cc of lipoaspirate using this method 28. Again, however, without the chemical bond release afforded by the enzymatic approach, the resultant cell composition is biased to be comprised of mainly white blood cells and certainly very few if any vascular endothelial or vascular progenitor cells which are contained within the the sublayers of the blood vessels.
While enzymatic methods yield higher cell counts, non-enzymatic methods are not without their merits. Collagenase for use in adipose tissue digestion tends to be fairly expensive. For use in a laboratory setting, where the number of progenitor cells may not necessarily be as important, non-enzymatic methods can provide a cost-effective alternative to acquire ADSCASCs. However, in 2013, Kakudo et al. conducted an animal based study which attempted to determine the optimal concentration of ADSCSVF cellss which should be used to supplement fat grafting 33. In this study, they suggested that the optimal concentration of cells was around 300,000 ADSCcellss per cc of graft tissue that was injected. They showed that at this concentration that they observed the best volume retention and lowest rates of oil cyst formation, inflammation, and fibrosis. It would be nearly impossible to achieve a cell density of this magnitude in the clinical setting using non-enzymatic methods based on reported cell yields. Therefore, while more expensive than non-enzymatic methods, the use of collagenase for isolation of SVF cells provides the best cell yield, and therefore is the most practical method for use in the clinical setting.
Safety of Residual Collagenase Activity:
The safety concerns about residual collagenase activity are all but negligible at the levels the we seeseen in our study. In a previous study conducted by our team, we demonstrated that the residual levels of collagenase observed using our manual isolation method were less than 0.01 Units of collagenase activity/cc of SVF isolated 30. This value drops even lower once the SVF cells are combined with the lipoaspirate for reinjection.
According to a 2013 study conducted by Chang et al., there were no concerns of toxicity relating to residual collagenase activity in ADSCSVF related procedures 34. They demonstrated the lack of toxicity in vivo using a mouse model. Mice were injected with a fat graft containing ADSCSVFs which had been isolated using collagenase. Mice were carefully monitored over 4 weeks, and then dissected for histopathological analysis. There were no significant changes observed between treatment and control group in this study. In addition, Chang et al. demonstrated that levels of residual collagenase activity are negligible so long as at least 3 washes of the SVF cells are conducted following tissue digestion.
In 2009, the Arthritis Advisory Committee issued a briefing document on Collagenase Clostridium histolyticum 35. In the document, they gave an extensive review of clostridial collagenase, mainly as it pertains to use in the drug Xiaflex (AA4500) for Dupuytren’s contracture. They reviewed both clinical and non-clinical evidence, which overwhelmingly supported the safety of collagenase. Three animal based studies that were reviewed showed that after local injection with clostridial collagenase there was no systemic toxicity and there was only a small amount of systemic exposure which resulted only if the collagenase was administered into highly vascular areas 36–39. Another animal based study of collagenase studied the effects of systemic circulation of collagenase by administering collagenase by IV to rats 35. In this study, it was noted that when collagenase was detected in systemic circulation that there was no accumulation following repeated dosing and it was cleared rapidly from the system. When administered intravenously at a high dose of 0.29 mg/animal, which is equivalent to almost 22 times the clinical dose of Xiaflex, class I collagenase was not detectable after 30 min and class II was not detectable after 2 hours. Overall, collagenase was determined to have a very low level of toxicity 40–42.
The levels of residual collagenase activity observed in our study (<0.01U >) are significantly lower than other collagenase based products which have been approved by the FDA, specifically Xiaflex and Collagenase Santyl. Santyl is a collagenase based ointment (250U/g) which is topically applied for enzymatic wound debridement 43,44. Xiaflex is a highly concentrated injection of collagenase (~ 3600 U/dose) used to treat Dupuytren’s contracture, a contracture of the hand due to palmar fibromatosis 45–47, and Peyronie’s disease, a similar contracture located in the penis 48,49. Xiaflex is administered by a direct subcutaneous injection into the site of contracture. Both of these products, Xiaflex and Santyl, underwent a high level of safety testing and were deemed safe by the FDA. The levels of collagenase activity observed in our study were thousands of times lower than those used in Santyl and Xiaflex. While only some comparison can be made between Santyl, Xiaflex and our use of collagenase because they are administered in different manners, it does offer some insight into the levels of collagenase activity that the FDA has deemed safe for human use[9] .
Conclusions:
As interest in fat grafting has grown in recent years, cell assisted lipotransfer has become a promising alternative for achieving superior results in fat grafting procedures. Our results demonstrate that using a non-automated, collagenase based procedure for the isolation of pluripotent stem cells from adipose tissue is indeed a safe and effective method which can be conducted at the point of care without added risk when compared to normal fat grafting procedures. Our results further supports the safety of cell-assisted lipotransfer and an expanded use of this emerging technology in the clinical setting.
While you may lose 10–15% of stromal vascular fraction cells during lipoaspiration that you would otherwise obtain if you digested whole lipectomy I am not sure I would call this a significant depletion. And after you wash away the disrupted tissue, the cells that remain associated with the intact adipose fat graft parcels after lipoaspiration is not significantly different on a stem cell per unit mass basis than that found within intact adipose prior to aspiration.
Joel, “stem cells” has a very specific connotation as referring to the adherent culture expanded cells capable of trilineage differentiation in vitro. It is not accurate to refer to the collective collection of stromal vascular cells which are comprised of many different cell types as “Stem cells”. It discredits your message in doing so. Might I suggest “stromal regenerative cells” or alternatively “stromal vascular progenitors” instead as terms which may be understood to be more than one cell type?
Again refers to the culture expanded phenotype. The frequency of these cells in a primary isolate is 1% or about 2,500 cells per gram of washed lipoaspirate
Okay, I would suggest using this phrase throughout.
“ASC” is the accepted acronym adopted by IFATS and the ISCT. I would use that instead.
Adipose derived regenerative cells was a phrase we coined at Cytori in 2005 to refer to stromal vascular fraction cells, not the cultured ASCs. Be careful not to use this phrase to refer to the cultured ASCs so that confusion is not generated in the literature.
Should name to the source/ and product name since this is a key element of the paper that you are assessing.
If you have the data, would be interesting to note the amount of cells recovered from male tissue versus female. This was something that we were going to publish at Cytori but never got around to. Would be interesting to see if you saw the same difference in cell yield (males being less)
Something we also thought about when I was at Cytori was the possibility that a little residual collagenase may help disrupt fibrotic matrix in the adipose transplant site and thereby helped create space for revascularization and integration of the adipose tissue. May want to mention this if you think it is worth doing so.
One final area of safety concern you might bring up is the level of neutral proteases (which are non-specific and can affect proteins on the cell surface. The point to make is that an understanding of the purity of collagenase is also important and is something that users must consider. However, your studies would support that even these are not a safety issue (at least in the enzyme and wash steps that you used for your process).
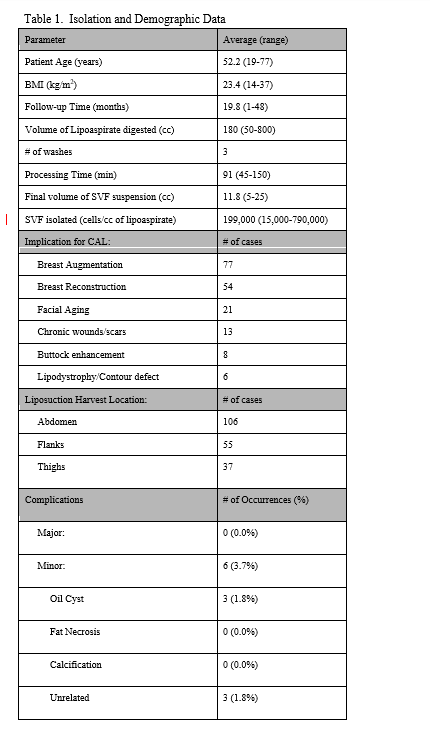
Figure 1 (a), (b): (a) Subject desired breast reconstruction in order to restore breast symmetry and improve cosmetic appearance after partial mastectomy(??) of the right breast. (b) A ?? flap was used accompanied by autologous SVF enhanced fat grafting which restored symmetry.

Figure 2 (a), (b): (a) Subject presented with hypoplastic breast and desired cosmetic augmentation without implants. Subject was injected with an SVF-enhanced autologous fat graft. (b) After grafting, the breasts were significantly larger while still presenting with a natural appearance and feeling.
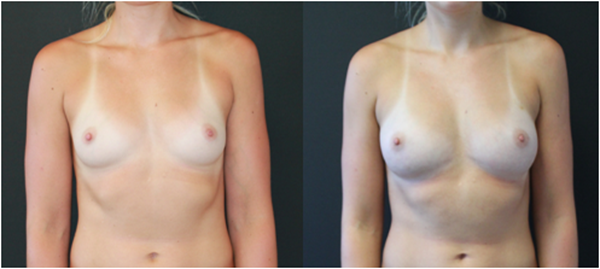
Figure 3 (a), (b): (a) Male age ## presented with signs of facial aging including malar and buccal wasting. Face was injected with an autologous SVF-enhanced fat graft to the cheeks and jaw. (b) After ## weeks/months the subjects face showed a fuller and younger appearance.

Figure 4 (a), (b): (a) Subject had a contour deformity which presented as a concave area on the right buttocks resulting from a complication from an injection which the subject received as a child. (b) The subject was injected with an autologous SVF-enhanced fat graft and after ## months, the deformity was no longer visible.
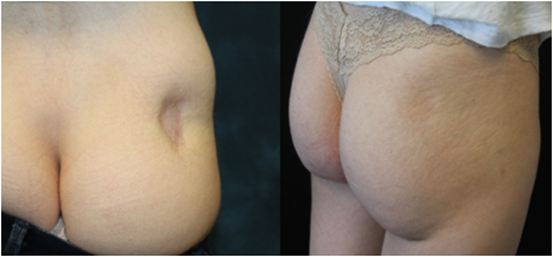
Figure 5 (a), (b), © : (a) A 73-year old woman with a chronic wound which presented as non-healing for 22 months (b) The wound was injected with ??cc of an autologous SVF-fat mixture generated at the point of care. © The wound was cleared after 9 weeks post-op.
References (in order for now)
1. Delay E, Garson SM, Tousson G et al. Fat injection to the breast: technique, results and indications based on 880 procedures over 10 years. Aesthet J Surg. 2009;29:360–76.
2. ASPRS Ad-Hoc Committee on New Procedures Report on autologous fat transplantation. Plast Surg Nurs. 1987;7:140–1.
3. Veber M, Tourasse C, Toussoun G et al. Radiographic Findings after Breast Augmenetation by Autologous Fat Transfer. Plast. Reconstr. Surg. 2011;127:1289.
4. Nagashima T, Hasimoto H, Oshida K et al. Ultrasound detection of mammographically detected microcalcifications in patients with ductal carcinoma in situ of the breast. Breast Cancer. 2005;12:216–220.
5. Rubin JP, Coon D, Zuley M et al. Mammographic Changes after fat transfer to the breast compared with changes after breast reduction: a blinded study. Plast. Reconstr. Surg. 2012;129:1029
6. Fiaschetti V, Pistolese CA, Fornari M et al. Magnetic resonance imaging and ultrasound evaluations after breast autologous fat grafting combined with platelet-rich plasma. Plast. Reconstr. Surg. 2013;132:498e.
7. Parikh RP, Doren EL, Mooney B et al. Differentiating fat necrosis from recurrent malignancy in fat-grafted breasts: an imaging classification system to guide management. Plast. Reconstr. Surg. 2012;130:761–72.
8. Kneeshaw PJ, Lowry M, Manton D et al. Differentiation of benign from malignant breast disease associated with screening detected microcalcifications using dynamic contrast magnetic resonance imaging. Breast. 2006;15:29–38.
9. Gutowski KA. Current applications and safety of autologous fat grafts: a report of the ASPS fat graft task force. Plast. Reconstr. Surg. 2009;124(1):272–80.
10. Suga H, Eto H, Aoi N et al. Adipose tissue remodeling under ischemia: death of adipocytes and activation of stem/progenitor cells. Plast. Reconstr. Surg. 2010;126:1911–23.
11. Eto H, Kato H, Suga H et al. The fat of adipocytes after nonvascularized fat grafting: evidence of early death and replacement of adipocytes. Plast. Reconstr. Surg. 2012;129:1081–92.
12. Kato H, Mineda K, Eto H et al. Degeneration, regeneration and cicatrization after fat grafting: dynamic total tissue remodeling during the first 3 months. Plast. Reconstr. Surg. 2014;133:303e-313e.
13. Yoshimura K, Sato K, Aoi N, Kurita M, Hirohi T, Harii K. Cell-assisted lipotransfer for cosmetic breast augmentation: supportive use of adipose-derived stem/stromal cells. Aesthetic Plast Surg. 2008;32(1):48–55.
14. Yoshimura K, Shiguera T, Matsumoto D et al. Characterization of freshly isolated and cultured cells derived from the fatty and fluid portions of liposuction aspirates. J Cell. Physio. 2006;208:64–76.
15. Ude CC, Sulaiman SB, Min-Hwei N et al. Cartilage regeneration by chondrogenic induced adult stem cells in osteoarthritic sheep model. Plos One. 2014;9(6):e98770
16. Planat-Bernard V, Silvestre JS, Cousin B et al. Plasticity of human adipose lineage cells towards endothelial cells: physiological and therapeutic perspectives. Circulation. 2004;109:656–63.
17. Rehmam J, Traktuev D, Li J et al. Secretion of angiogenic and antiapoptotic factors by human adipose stromal cells. Circulation. 2004;109:1292–98.
18. Naderi N, Wilde C, Haque T et al. Adipogenic differentiation of adipose-derived stem cells in a 3-dimensional spheroid culture (microtissue): implications for the reconstructive surgeon. J Plast. Reconstr. Aesthet. Surg. 2014;pii: S1748–6815(14)00434–3
19. Sahil KK, Katz AJ et al. Review of the adipose derived stem cell secretome. Biochimie. 2013;95:2222–28.
20. Zuk PA, Zhu M, Mizuno H et al. Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Engineering. 2001;7:211–29.
21. Matsumoto D, Sato K, Gonda K et al. Cell-assisted lipotansfer: supportive use of human adipose-derived stem cells for soft tissue augmentation with lipoinjection. Tissue Engineering. 2006;12(12):3375–83.
22. Yoshimura K, Suga H, Eto H et al. Adipose-derived stem/progenitor cells: roles in adipose tissue remodeling and potential use for soft tissue augmentation. Regen. Med. 2009;4(2):265–273.
23. Kølle SF, Fischer-nielsen A, Mathiasen AB, et al. Enrichment of autologous fat grafts with ex-vivo expanded adipose tissue-derived stem cells for graft survival: a randomised placebo-controlled trial. Lancet. 2013;382(9898):1113–20.
24. McCarthy RC, Breite AG, Dwulet FE. Biochemical Analysis of Crude Collagenase Products used in Adipose Derived Stromal Cell Isolation Procedures and Development of a Purified Tissue Dissociation Enzyme Mixture. 2010. Accessed November 3, 2014. http://www.vitacyte.com/wp-content/uploads/2009/01/ifats-vitacyte.pdf
25. Eckhard U, Schӧnauer E, Ducka P et al. Biochemical characterization of the catalytic domains of three different clostridial collagenases. Biological Chemistry. 2009:390(1);11–18.
26. Matsushita O, Koide T, Kobayashi R et al. Substrate recognition by the collagen-binding domain of Clostridium histolyticum class I collagenase. J Biol. Chem. 2001;276(12): 8761–70.
27. Matsushita O, Jung CH, Minami J et al. A study of the collagen-binding domain of 116-kDa Clostridium histolyticum collagenase. J Biol Chem. 1998; 273:3643–48.
28. Shah FS, Wu X, Dietrich M et al. A non-enzymatic method for isolating human adipose-derived stromal stem cells. Cytotherapy. 2013;15:979–985.
29. Markarian FM, Frey GZ, Silveira MD et al. Isolation of adipose-derived stem cells: a comparison among different methods. Biotechnol Lett. 2014;36:693–702.
30. Dr Joel Aronowitz , Ellenhorn JD. Adipose stromal vascular fraction isolation: a head-to-head comparison of four commercial cell separation systems. Plast. Reconstr Surg. 2013;132(6):932e-9e.
31. Raposio E, Caruana G, Bronomini S et al. A novel strategy for the isolation of adipose-derived stem cells: minimally manipulated adipose-derived stem cells for more rapid and safe stem cell therapy. Plast. Reconstr. Surg. 2014;133(6):1406–9.
32. Baptista LS, do Amaral RJ, Carias RB et al. An alternative method for the isolation of mesenchymal stromal cells derived from lipoaspirate samples. Cytotherapy. 2009;11(6):706–15.
33. Kakudo N, Tanaka Y, Morimoto N et al. Adipose-derived regenerative cell (ADRC)-enriched fat grafting: optimal cell concentration and effects on grafted fat characteristics. J Trans. Med. 2013;11:254–63.
34. Chang H, Do BR, Che JH et al. Safety of adipose-derived stem cells and collagenase in fat tissue. Aesthetic Plast Surg. 2013;37(4): 802–08.
35. AAC Briefing Document for Collagenase Clostridium Histolyticum (AA4500) September2009.Accessed October 7, 2014. http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/ArthritisDrugsAdvisoryCommittee/UCM182015.pdf
36. Miyabayashi T, Lord PF, Dubielzig RR et al. Chemonucleolysis with collagenase. A radiographic and pathologic study in dogs. Vet Surg. 1992;21:189–94.
37. Friedman K, Pollack SV, Manning T et al. Degradation of porcine dermal connective tissue by collagenase and by hyaluronidase. Br J Dermatol. 1986;115:403–408
38. Bromley JW, Hirst JW, Osman M et al. Collagenase: an experimental study of intervertebral disc dissolution. Spine. 1980;5(2):126–32.
39. Bromley JW. Intervertebral discolysis with collagenase. Arzneimittelforschung. 1982;32(10a):1405–8.
40. Zook BC, Kobrine AI. Effects of collagenase and chymopapain on spinal nerves and intervertebral discs of Cynomolgus monkeys. J Neurosurg. 1986;64:474–83.
41. Sussman BJ, Bromley JW, Gomez JC. Injection of collagenase in the treatment of herniated lumbar disk: Initial clinical report. JAMA. 1981;254(7): 730–32.
42. Garvin PJ. Toxicity of collagenase: the relation to enzyme therapy of disk herniation. Clin. Orthop. Relat. Res. 1974;101:286–91.
43. Shi L, Carson D. Collagenase Santyl ointment: A selective agent for wound debridement. J Wound Ostomy Continence Nurs. 2009;36(65):512–16.
44. Exploring Clinical Data for Collagenase Santyl Ointment. Santyl website. Accessed November 4, 2014. http://www.santyl.com/hcp/clinical-data
45. Nunn AC, Schreuder FB. Dupuytren’s contracture: emerging insight into a viking’s disease. Hand Surg. 2014;19(3):481–90.
46. Gilpin D, Coleman S, Hall S et al. Injectable collagenase clostridium histolyticum: a new nonsurgical treatment for Dupuytren’s disease. J Hand Surg Am. 2010;35(12):2027–38.
47. Sood A, Therattil PJ, Paik AM et al. Treatment of Dupuytren’s contracture with injectable collagenase in a veteran population: a case series at the department of veteran affairs new jersey health care system. Eplasy. 2014;14:e13
48. Egui Rojo MA, Moncada Iribarren I, Carballido Rodriguez J et al. Experience in the use of collagenase histolyticum in the management of peyronie’s disease: current data and future prospects. Ther Adv Urol. 2014;6(5):192–7.
Gelbard M, Goldstein I, Hellstrom WJ et al. Clinical efficacy, safety and tolerability of collagenase clostridium histolyticum for the treatment of peyronie disease in 2 large double-blind, randomized, placebo controlled phase 3 studies. J Urol. 2013;190(1):199–207.
